(0 rating, 2 votes)
(0 rating, 2 votes)
ACSO08_XRayPart1-placement2-800
My partner and I just finished teaching an advanced pistol class. One of our students came over to me, frowning. “Doc, I feel a lot better about my shooting skills after this class,” he said quietly. “But I’m still unclear about one thing. Where should I be aiming to put my opponent down?”
If this had been one of my civilian CCW students I wouldn’t have been surprised by the question. But this was a veteran cop with a successful officer-involved shooting (OIS) under his belt. Being an ER doc and firearms instructor, I’d been asked this question hundreds of times, so I gave him the short version of my recommendations.
“For this reason, among others, train to aim at the high mediastinum.
This is supported by the experience of guys at the sharp end of the
spear in highly lethal environments such as South Africa, the
Middle East and parts of Asia.”
This cop’s question highlights a glaring deficiency in police firearms training.
Outside of a few instructors, such as Louis Awerbuck and Massad Ayoob, realistic training on where to shoot the bad guy is rare.
Scoring zones on most police qualification targets have little or no relationship to the vital anatomy of the human body. Paper targets present the opponent facing squarely toward the firing line, but OIS data show frontal target presentation is uncommon.
While touting qualification scores in the 80 percent range or better, most law enforcement agencies document OIS handgun hit ratios between 9 and 65 percent. It doesn’t take a rocket scientist to see there’s a critical gap between firearms training and OIS performance.
SEEKING A SOLUTION
Over a decade ago, I tried to devise paper targets with anatomic overlays, but realized simply moving the shooter two steps to one side rendered the anatomic geometry invalid. A lot of paper targets with anatomic outlines have come out since, but they all have the same flaw. Surface outlines are only relevant from one point in space —directly in front of the target.
Then I tried building a three-dimensional human target, but discovered making it anatomically correct was too costly to shoot, and cheaper alternatives were anatomically useless.
The solution came to me as I mentored the 12-year-old son of a non-hunting neighbor who wanted to learn to hunt. I’d shown Kyle photos of deer with the vitals outlined — in frontal and side presentations. Early in the season I shot a doe and Kyle watched as I field-dressed it, demonstrating the location of the heart, lungs and great vessels. He clearly got the picture, because the next morning he placed a bullet perfectly into the chest of a buck quartering away at 85 yards —dropping it in its tracks.
Most importantly, Kyle was able to tell me before we dressed the deer what the path of his bullet through the deer would likely be, and when we opened it up he was right.
If a 12-year-old kid can learn the 3-D anatomy of a deer, why can’t a cop learn the 3-D anatomy of the human body just as easily? And, if cops could know precisely where to shoot, wouldn’t that translate into better hits on suspects?
Over the next two years with a lot of input from cops and other doctors, I developed the 3-D targeting method called Tactical Anatomy.

B27 qualification target closeup
B27 qualification target back view
3-D TARGET VISUALIZATION
Three challenges need to be met in training cops to be 3-D shooters. They need to learn what are the vital hit zones. They need to learn to see these zones in three-dimensional space, and they need to merge their existing firearms proficiency with these new 3-D visualization skills.
WOUNDS AND INCAPACITATION
There are a lot of myths regarding gunshot wounds (GSWs) and incapacitating the human body spawned by Hollywood and the Internet.
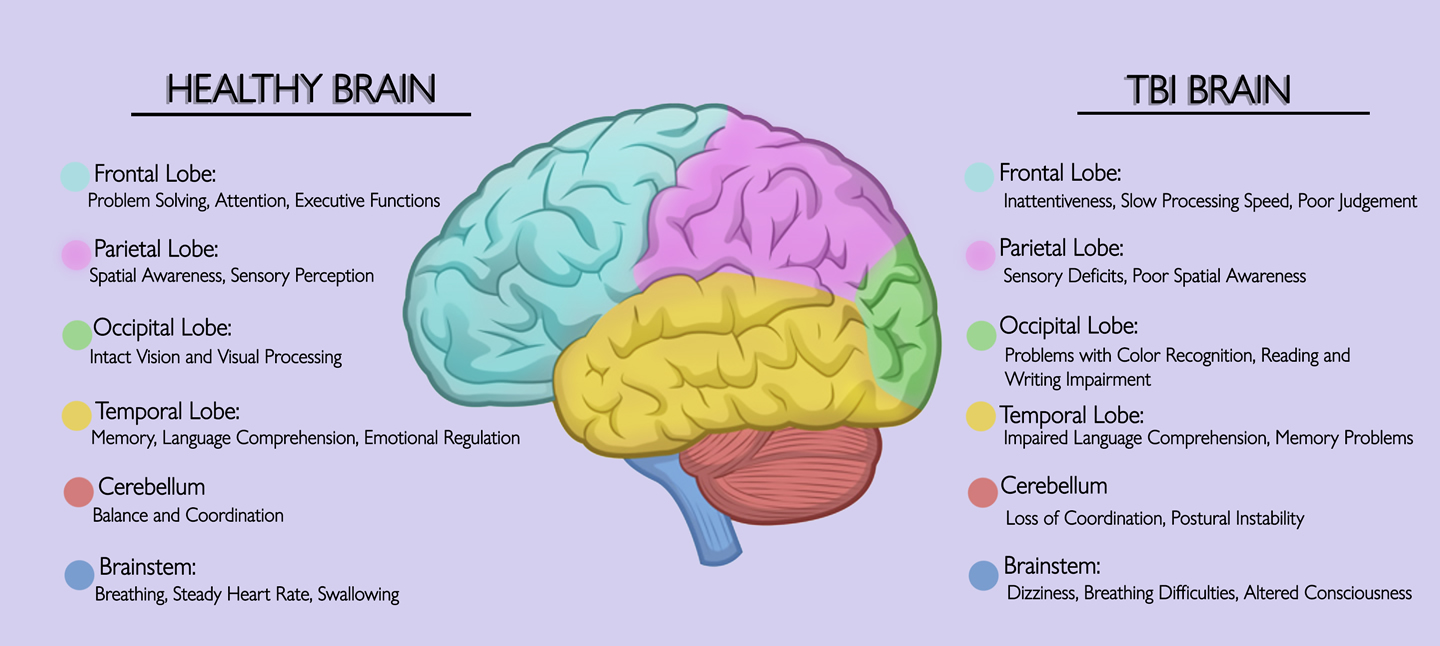
There are only two reliable means of shutting down the human body pronto: destruction of the Central Nervous System (CNS) — the brain and upper spinal cord — and catastrophic blood loss.
Skeletal system destruction is a special third case, which I will get into in the next article in this series.
The bottom line is a cop’s bullets need to destroy the CNS or shut down its supply of oxygen to stop a suspect’s violent acts immediately. These are the vital zones upon which we’ll concentrate.


MEETING THE CHALLENGES
The first challenge isn’t hard to meet. Using anatomic drawings, x-rays and photos, the anatomy of vital structures is easily illustrated. Using different views— front, side and oblique — we begin to form a construct.
The second challenge is to help change the view of anatomy from flat, two-dimensional drawings into a 3-D model. It can’t be bought from a mail-order house — it’s something we have to create in the mind.
The solution lies in the fact that human beings function in three-dimensional space 24-7. Two-dimensional anatomic drawings are artificial and we subconsciously know this. All we have to do is show a way to turn on the 3-D brain. In learning theory, it’s called a cognitive bridge.
We create this cognitive bridge in the classroom by using a simple yet highly effective method. We generate a 3-D model by transcribing the 2-D anatomy onto an assistant while refer-ring to anatomic illustrations. This demonstrates relationships between the vital zones and surrounding structures.
The first time I used this method, I almost saw lightbulbs flashing on over the class members’ heads.
The third challenge, merging existing handgun proficiency with 3-D visualization, is accomplished through a series of exercises using dummy guns, laser sights and computer simulators such as FATS or MILO. The training can be accomplished in about eight hours and it’s proven to be highly retainable.
CENTER OF MASS MYTH
The concept of “center of mass” (COM) as the primary target in an OIS is virtually dogmatic in police firearms training. But ask 10 different cops to write down their definition of COM, and you’ll get 10 different answers. It’s not a term you’ll find in anatomy textbooks.
Center of mass means shoot “somewhere in the middle” and it’s a hopelessly vague term. Training cops to aim for the middle guarantees misses and/or ineffective hits.
As the hunter’s axiom goes, “aim small, miss small” and if you aim big, you’ll miss big. Even if we define COM as the chest, two-thirds of that anatomic region is lungs and lung hits don’t cause rapid incapacitation.
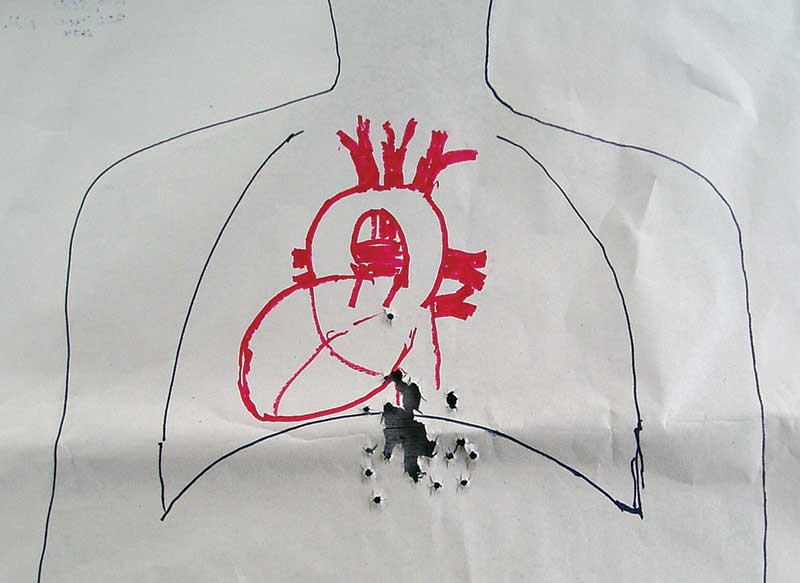
Train to visualize the heart and the cluster of great vessels immediately above the heart and make that your primary target. This zone is called the mediastinum. When viewed three-dimensionally, it’s roughly the size and shape of a quart milk bottle. This large target zone is highly vulnerable to handgun bullets, particularly the top (atria) of the heart and the great vessels.
“Several agencies in these places train their CQB personnel to shoot the high mediastinum first and it’s devastatingly effective.”
A cardiac surgeon I know once assured me if a breathing patient with a bullet in his heart hit my ER doors —not uncommon in inner city hospitals— Charlie could almost guarantee he’d save the patient’s life in the OR. But, if the GSW involved the atria or great vessels, the chance of survival is almost zero. The heart is a tough, muscular organ and a hole in it can be easily sutured shut. The thin-walled great vessels aren’t nearly as resilient. As Charlie put it, “Suturing the aorta or vena cava is like trying to sew a fart to a moonbeam.”
An armed opponent shot in the heart may be able to keep fighting long enough to kill you. If your bullets take out the great vessels — the fight will be over in seconds.
For this reason, among others, train to aim at the high mediastinum. This is supported by the experience of guys at the sharp end of the spear in highly lethal environments such as South Africa, the Middle East and parts of Asia. Several agencies in these places train their CQB personnel to shoot the high mediastinum first and it’s devastatingly effective.
ONE LESS DECISION
Training to visualize the vital zones of the human body and to see these zones in three dimensions has obvious benefits for the patrol officer. If con-fronted by a lethal threat, he has one less decision to make in his OODA loop as he brings his sidearm to bear. He reflexively knows where his bullets need to go — from any angle of presentation. The consequence is more bullets hitting the real target — the suspect’s vital anatomy.
In the next article, we’ll look at two other vital zones of the body, and reality-based training methods that can fine-tune your CQB skills.