(+6 rating, 6 votes)
(+6 rating, 6 votes)
feature-hemorhage_6779
When I went through the 1st Responder curriculum (a prerequisite for EMT), in 1987, we were taught A-B-C for Airway, Breathing, Circulation.
Next was M-A-R-C-H: Massive Hemorrhages, Airway, Respiration, Circulation, and Hypothermia. I can’t recall hearing it in my second complete EMT class (2001) or in Combat Life Saver (2004). I started hearing it frequently after 2010. Last year, I realized it had been a few years since I had received any in-depth medical training, and I needed to refresh my skills.
An hour here or there wasn’t enough.
At a recent veterans’ event, I shared a table with a gentleman who runs a local medical training business. His public classes focus on TECC – Tactical Emergency Casualty Care – the civilian version of Tactical Combat Casualty Care.
The Armory in Sandy, Utah, hosted his TECC for Active Bystanders course.
Bottom line? A well-presented class from an instructor with both clinical and field experience. He is an Army medic, an EMT turned paramedic, and now an emergency room tech, then ER nurse. I like the EDIP model for teaching hands-on skills: Explain, Demonstrate, Imitate, Practice. Iron Rescue’s curriculum does that.
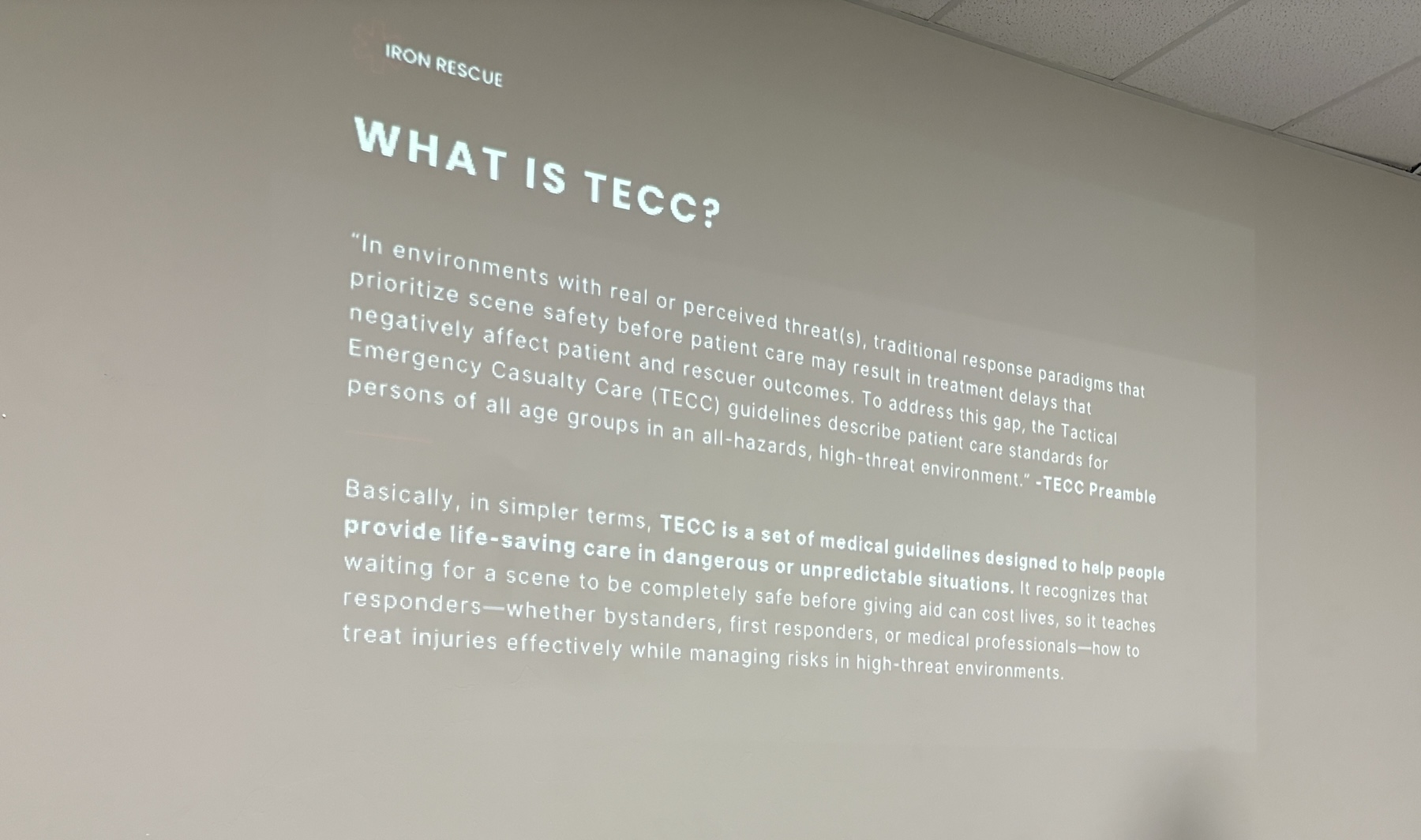
The What behind the Tactical Emergency Casualty Care curriculum.
The Why?
Medical emergencies happen around us a lot. These don’t have to be gunshot wounds. They can be accidents or medical conditions. For example, two range training situations I dealt with a few years after retiring from full-time L/E.
1st, a student was shooting around a barricade; they cleared the sights but not the muzzle. When they shot, the round struck the barricade, launching a significant amount of splinters and fragments into their face, penetrating their skin.
2nd, an older gentleman with a cardiac history displayed all the signs preceding a heart attack. Fortunately, I asked the right questions – like is pain radiating up and down your left arm? – We had to get him emergency medical care. Before class even started that day.
The class was made up of currently serving street cops and EMTs, gentlemen working in the trades, and me.
The What
We started by discussing the differences and similarities between TCCC and TECC. In Utah, this means treatment protocols are based on your current status, not your job.
There are three distinct phases; shifting back and forth is not uncommon. Direct Threat Care, Indirect Threat Care, and Evacuation.
During TECC, the priorities differ from law enforcement’s Priority of Life. Take care of yourself first, then your family or team, those around you, and finally the casualty. All that starts with ensuring your safety, be it by donning non-latex gloves first or suppressing the BadGuys gunfire.
Direct Threat Care involves getting yourself and others to safety. Mitigating the threat, however, is appropriate. Finally, stopping major hemorrhaging within a 30-second standard.
Indirect Threat Care includes scene safety, casualty assessment, and appropriate interventions (within your scope of practice). Monitor and re-assess your patients after treatment, then prepare for evacuation.
Evacuation is moving them to a staging area, definitive treatment, or transportation. This could be one or two-man carries or using a vehicle.
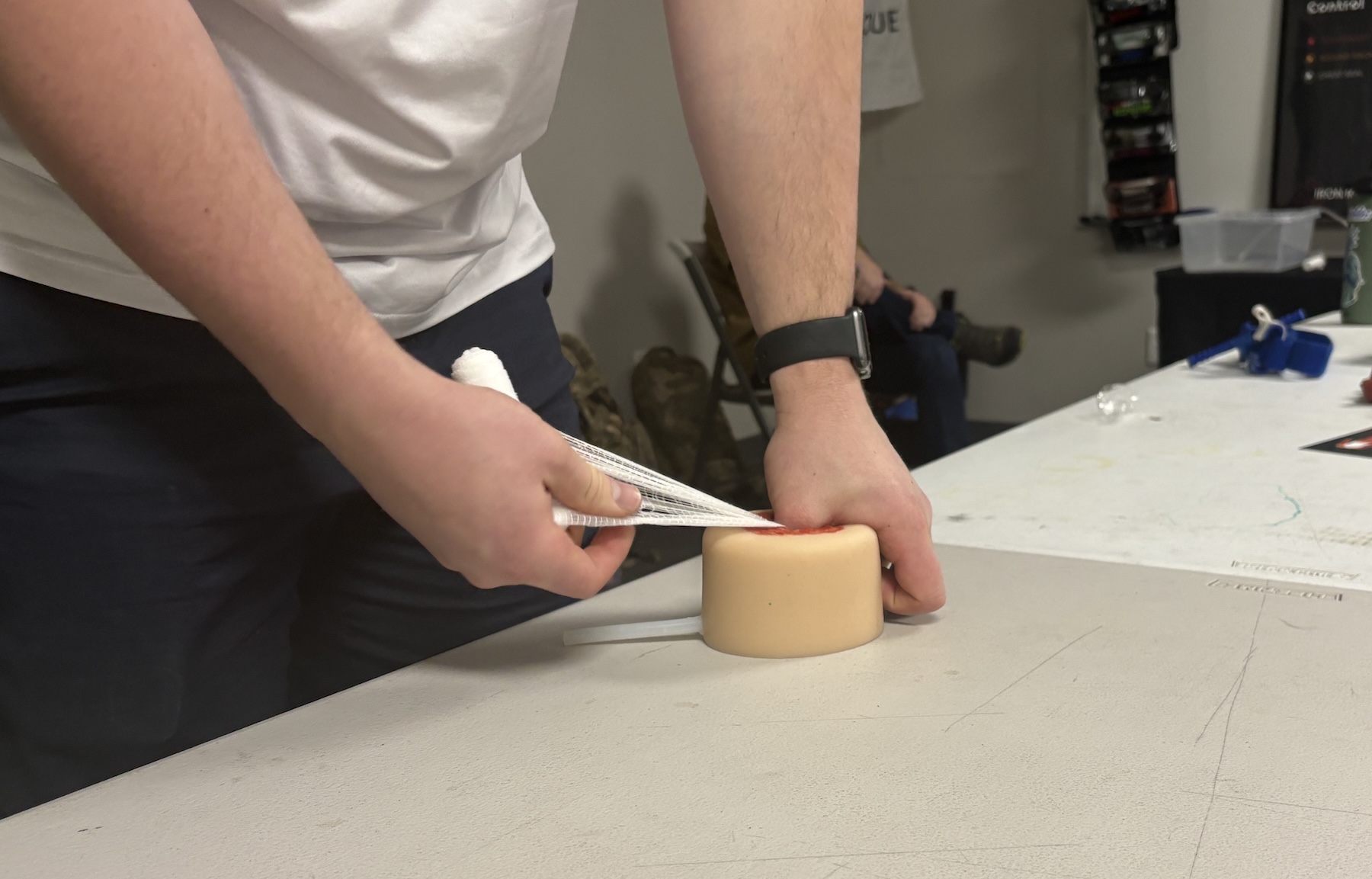
Easton is demonstrating how to pack a wound with rolled gauze so that you can apply direct pressure.
MARCH
M is major hemorrhaging. Look for blood pooling below them, then sweep their limbs and torso by raking with finger tips to find holes. Check the gloves after each body part and limb. Treatment is based on where the bleeding is – tourniquet limbs, pack gauze into the junctions, or seal the torso.
Spinal concerns are very different from those in my EMT program. Go take a TECC class.

A variety of tourniquets were shown and demonstrated. We used trainer versions of the CAT during the class.
We saw a variety of tourniquets and had numerous opportunities to practice their application.
Wound packing with regular and impregnated gauze was discussed and demonstrated. We practiced with two types of trainers: fake blood and clotting agents.
Pressure dressings were next up. They are not a second tourniquet and don’t need to be as tight. Checking the extremities for distal (far side) pulses after applying them is important.
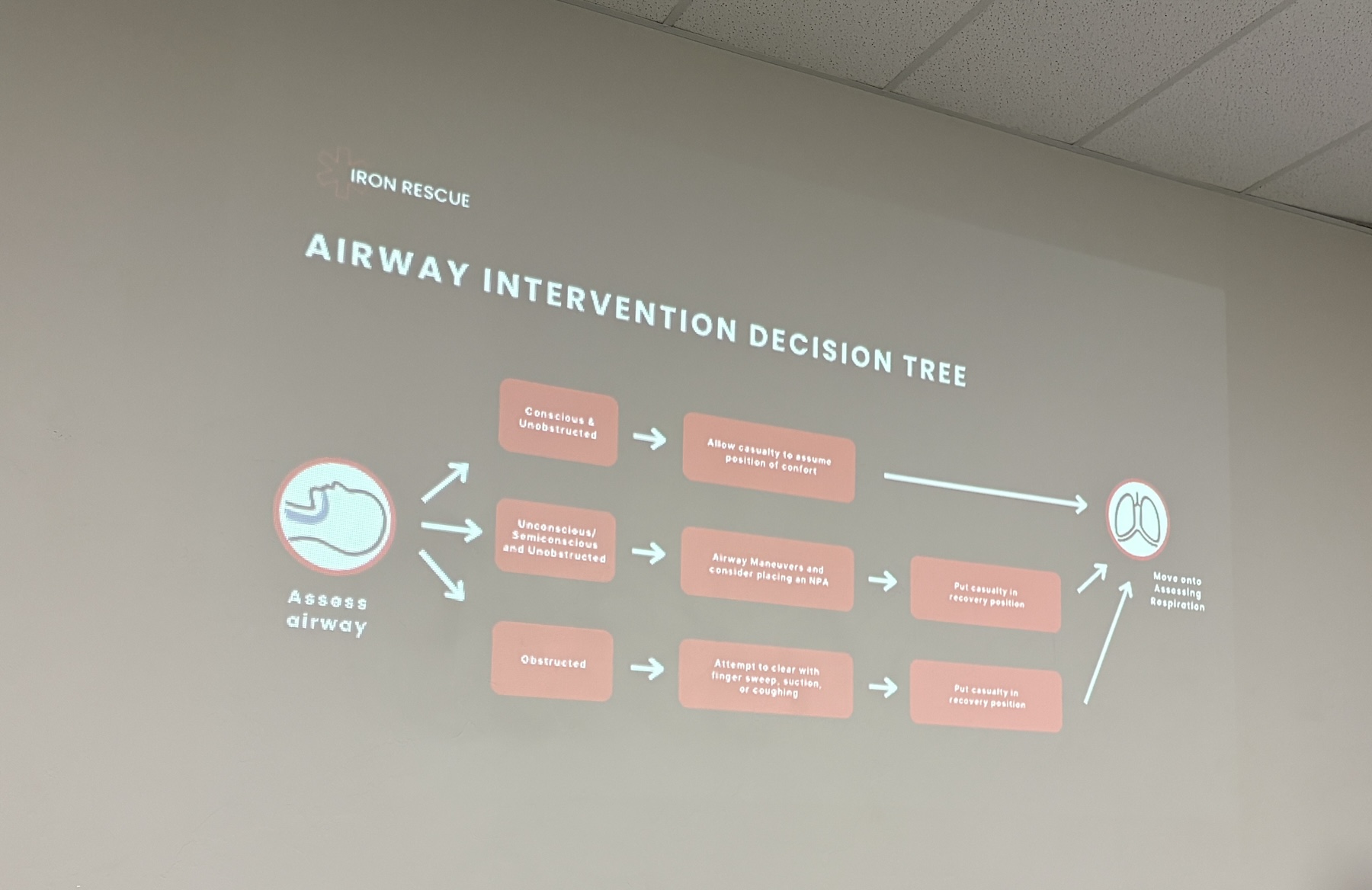
Working through the various possibilities you can encounter with a patient’s airway.
Airway
The head tilt/chin lift and the jaw thrust – for head/neck trauma – were both taught. No mechanical airways were taught.
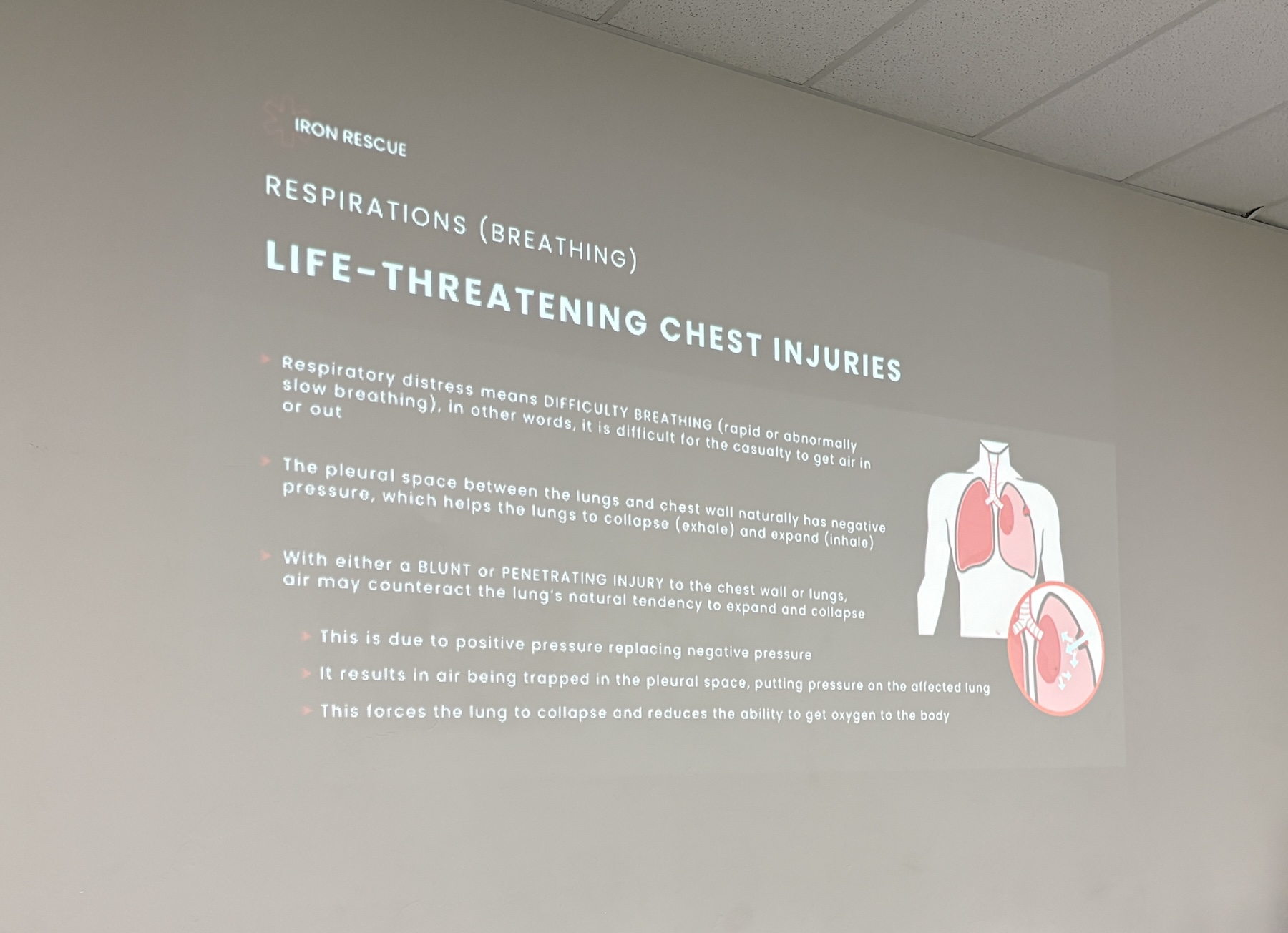
Discussion of the issues relating to the R – respiration – part of MARCH
Respiration
Ensure the airway structure is intact. If there are injuries or trauma to the chest, place them in a recovery position (on their side) with the affected lung down – keep the good lung up.
TECC recommends only using vented chest seals for the chest. If no vented seals are available, their direction is to leave it open in the continental US.
Pay attention to difficulty breathing, shortness of breath, cyanosis (lack of oxygen), and distended jugular veins.
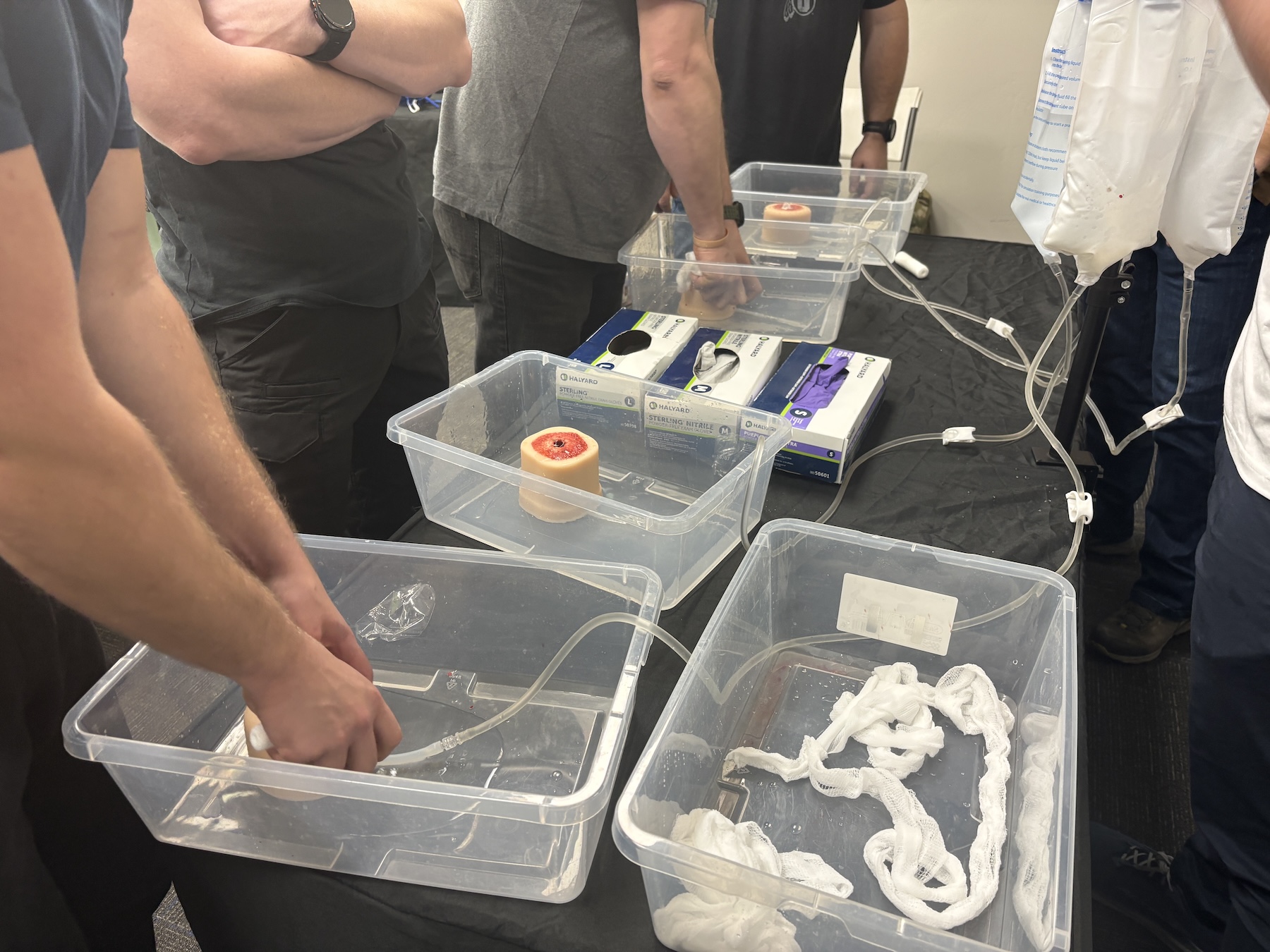
Pack the wound with the gauze, and keep the fluid inside. There’s a theme here – massive hemorrhage.
Circulation
Find their radial (wrist), femoral, or carotid pulses and use those to assess their blood pressure.
You’ll need to re-check tourniquets during this time and may need to retighten them.
Assessing their pelvic structure came next.

A little encouragement when practicing wound packing. Keep the water from flowing out of the trainer.
Hypothermia
Research shows a significant number of trauma patients die from this, regardless of the time of year or ambient temperature. It is the inability to regulate one’s body temperature. Preventing hypothermia was emphasized as being easier than re-warming them.
Heat loss through conduction, convection, evaporation, and radiation was covered.
Shock, both physical and mental, was addressed. Mitigation included cognitive and sensory grounding. One method was to name 5 things you can see, 4 you can hear, 3 you can touch, 2 you can smell, and 1 you can taste.
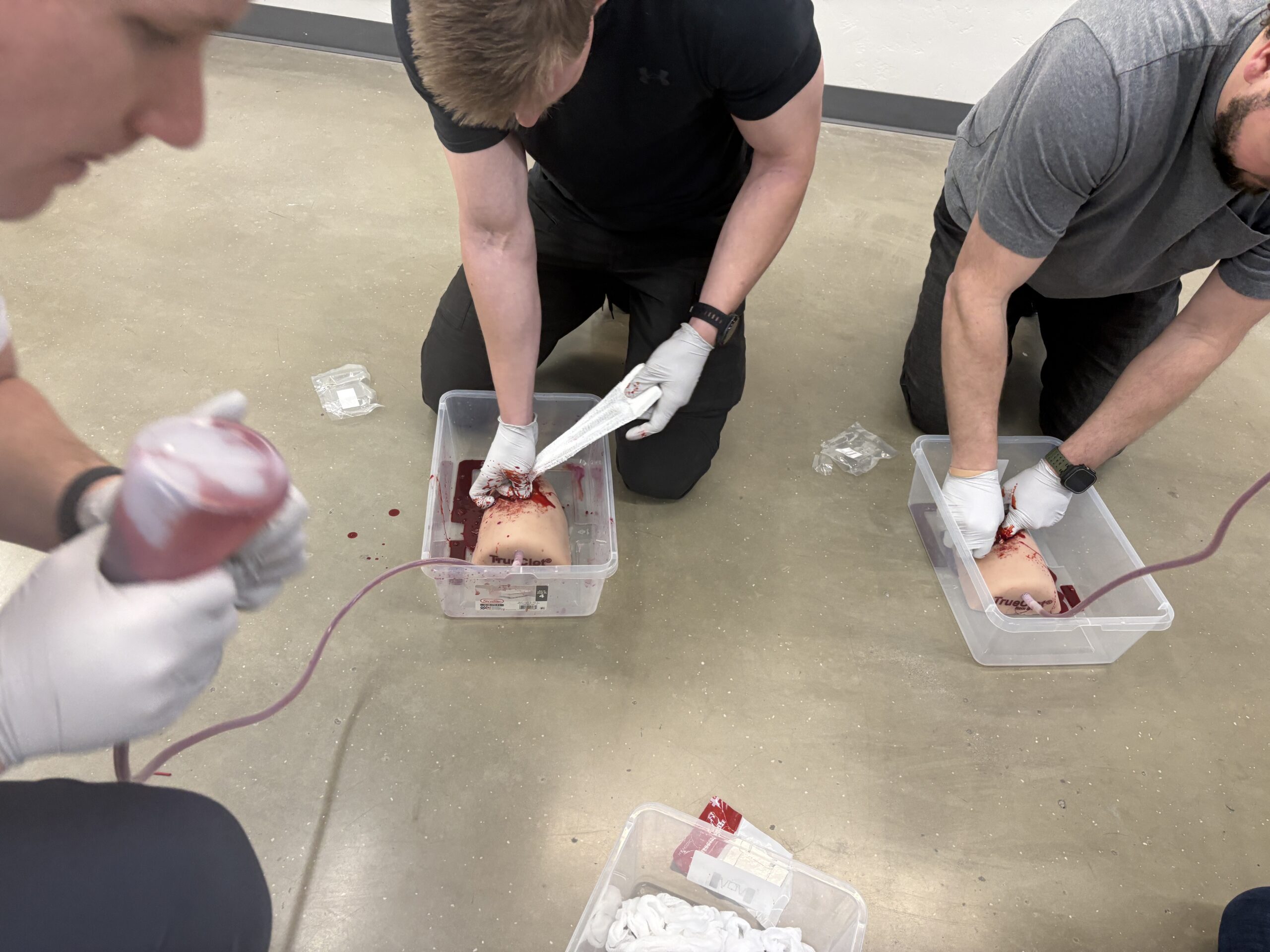
A thigh & gunshot wound simulator. Find the bleed, pack the wound, and keep the fake blood with the ability to clot inside. Go!
Age
We discussed treating the young and the old. All the TECC treatment and equipment recommendations are child-safe.
The same treatment algorithms apply to both.
Gear
If you didn’t like gear, you wouldn’t be reading this.
TECC doesn’t recommend specific products; they do provide specifications. Soon, the Committee on TCCC will do the same. Essentially, giving you the left- and right-hand limits of acceptability.
Your kit should include two tourniquets, chest seals, gloves, gauze (hemostatic & plain), pressure dressings, shears, tape, and boo-boo stuff.
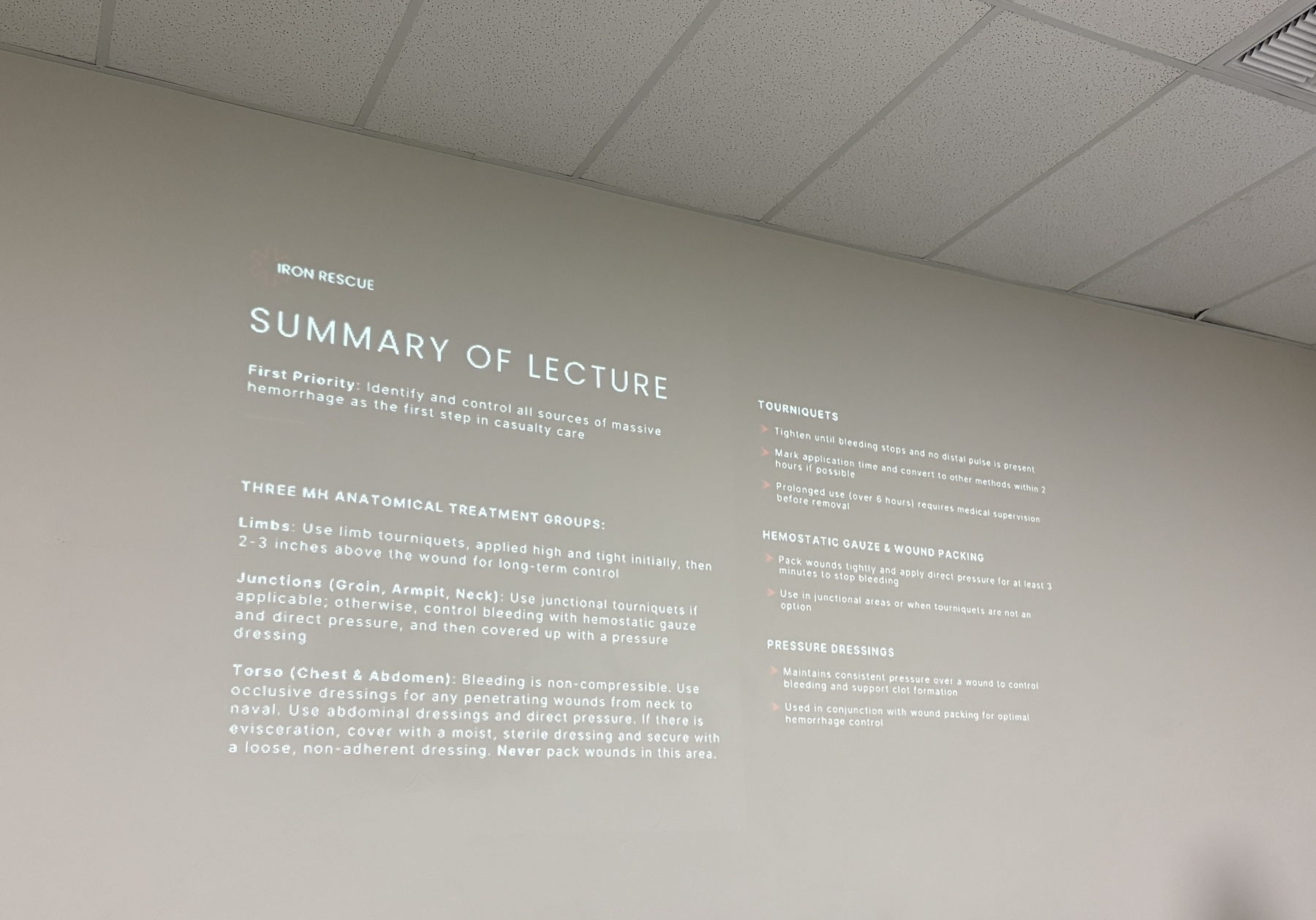
Each lecture section was re-capped before heading on to the next subject.
Final Thoughts
We all need competently presented medical training. Find a nearby provider who fits that description.
I paid for this class, and there was no expectation of a positive review.
RESOURCE: