(-1 rating, 1 votes)
(-1 rating, 1 votes)
ACND08_XRayPart2-anatomy4-800
At a 2007 law enforcement training conference the wife of one of the attendees criticized me sharply for training cops in Tactical Anatomy. She contended, quite rightly, if cops shoot more effectively more felons are going to be killed.
“Excuse me,” I replied. “What part of the term “deadly force” don’t you understand?”
I went on to explain, as a physician, I’m supposed to be a healer. Critics assert my training methods violate medical ethics. I respond with these words from the Hippocratic Oath: “Do good, but first do no harm”.
To heal a patient, sometimes a doctor needs to cause harm. There is no question that cutting a man’s belly open causes him harm. But to not cut in order to remove a ruptured appendix imposes a death sentence from infection — obviously a greater harm. This illustrates the Doctrine of Competing Harms: when faced with two harmful options, the physician must choose the less harmful one.
I justify training cops to shoot with X-ray vision by the same doctrine: Not teaching 3D targeting skills results in more cops’ bullets missing — in turn more criminals will be able to return fire — by inaction this would cause greater harm to good people in uniform. And frankly, I’ll pick the cop over the bad guy every time.
Cops already understand the Doc-trine of Competing Harms, or they wouldn’t be doing the job. We all learned in early childhood it’s wrong to hit, stab, or shoot people. But society expects cops to do exactly that when circumstances require, because society operates under the same ethical doc-trine. Society doesn’t want cops to enjoy employing deadly force, but it expects them to be good at it. And get-ting cops good at it is what Tactical Anatomy is all about.
ALTERNATIVE TARGETING
In the first article of this series, we discussed why the upper mediastinum is the recommended primary target for cops facing a deadly opponent. But sometimes there’s a need for an alternative.
Spring, 2007: cops in a Midwestern city responded to a call to a man threatening with a knife. The knife brandishing subject threatened to kill the officers con-fronting him. He charged and was shot in the chest several times with no apparent effect. One of the officers fired a round into the subject’s lateral pelvis, shattering the pelvis and hip joint. He crashed to the ground and was disarmed and subdued.
Surgeons were able to fix the holes in his chest, but were unable to repair the damage to the nerves and blood vessels in his pelvis and his leg was subsequently amputated at the hip.
This illustrates the need for alternative target solutions to the mediastinum. Even though the bullets had done severe damage to vital organs in his chest, the subject was able to continue his attack.

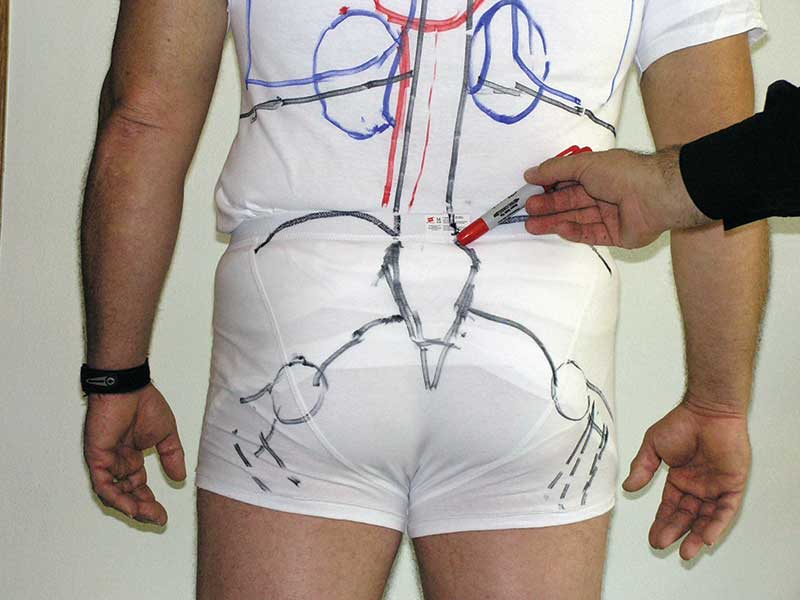
Pelvis and hip anatomy. Weight-bearing triangle is outlined on left in blue. General location of the vascular bundle of arteries of veins is outlined on right in red.
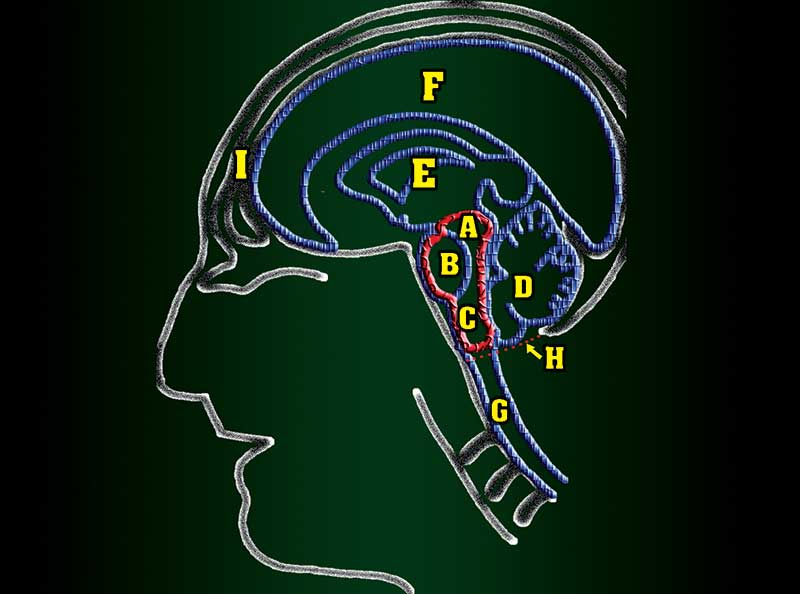
The brainstem consists of three primary structures: the midbrain (A), pons (B) and medulla oblongata (C), close to the cerebellum (D) which provides coordination and relays messages to the body through the spinal cord (G).
FAILURE DRILLS FAIL
We all know the term “failure drill”: fire a double-tap to center of mass, then fire a shot into the head zone of the target. Alternatively, we perform a “nonstandard response” (NSR) consisting of 5 or more rounds to COM.
But the reality is failure drills and NSRs often fail on the street. We’ve learned training to “double-tap-then-assess” is a recipe for getting cops killed (more on this in Part 3). Also, more and more felons are wearing body armor. We need to train our people in more reliable alternate targeting.
Gunfight circumstances may take the mediastinum and CNS vital zones off the menu. Consider the example above, or the North Hollywood bank robbery. In cases like these extreme distance, body armor, subject mobility or a combination of these take away the mediastinum and CNS as effective targets. That’s why I recommend the lateral pelvis as the first alternative target.
Note that I don’t say “the pelvis.” Like center of “mass”, the pelvis means different things to different people. Too many people think they can simply lower their sights down the midline, but between the navel and the ‘nads there’s nothing but intestines, and gut shooting a man won’t make him quit fighting. To make an incapacitating hit, you need to move your sights down and laterally to where the important stuff is.
So what exactly is the important stuff, anyway? First, the bones that transfer the weight of the torso down to the legs. Orthopedic surgeons call this the weight bearing triangle (Fig. 1). If these bones are shattered by a bullet, the subject is rendered physically incapable of remaining upright. Second, the large-bore arteries and veins supplying the legs run through this same area and actually represent a greater target area than the mediastinum.
I’ve trained to consider the lateral pelvis as the first alternate target zone for years. There are a lot of cases and studies backing this up. Recently Henk Iversen of Strike Tactical Inc., one of the most innovative trainers in America, told me he agrees.
Iversen’s extensive experience in military and SWAT duty in South Africa taught him personnel in CQB situations should use the lateral pelvis as a primary target. I’ve debriefed other guys who have spent time on the sharp end of the spear in The Sandbox who echo Iversen’s doctrine.
Anatomy of the bony pelvis (posterior view) on model at Tactical Anatomy class.

Doc illustrates location of the weight-bearing triangle on model in a Tactical Anatomy class in Florida, 2005.
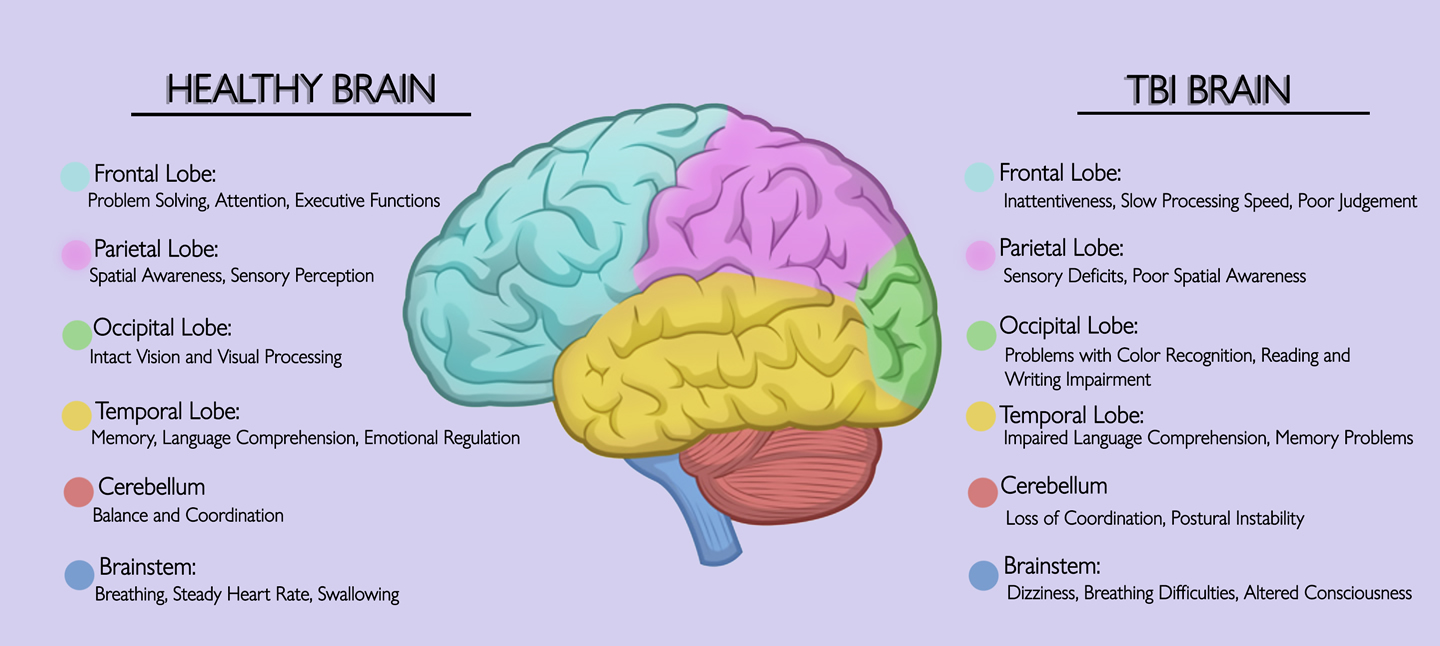
TAKE OUT COMMAND CENTER
The brain is fueled by oxygen. In a normal state, the brain has enough oxygen stores to maintain intentional action for 7-10 seconds even if its blood supply is cut off. In an excited state brought on by drugs or psychosis, greater oxygen stores may permit violent actions for 10-15 seconds or more.
But sometimes, such as a situation where a felon is holding a hostage at gunpoint, you don’t have ten seconds. You need to put him down now, and that means shutting down the central nervous system (CNS).
The problem is cops aren’t taught what part of the CNS they need to target in this situation. The vital zone is the brainstem, the relay station between conscious thought and purposeful motion. This zone is small, and deep inside the skull. A bullet through the brainstem will cause immediate incapacitation of the subject. Contrary to Hollywood mythology, a subject shot here won’t reflexively shoot the bystander he holds at gunpoint. His muscles will go limp and he will collapse.
While a high-power rifle bullet any-where in the brain is an almost certain fight-stopper, the lower energy of handgun bullets requires more precision. There are numerous cases of individuals with handgun bullets in their brains who continued to fight because a cop’s bullet did not take out the vital brainstem. Moreover, the cranium has a distinct curve to it, and — particularly handgun bullets — can literally bounce off the sloped bone. Precise aim is required, but any competent police marksman can make this shot within his confidence range.
The brainstem is a great alternative to the mediastinum. Despite being a small — and often a moving— target, in specific situations the brainstem is the best vital target zone and cops need to know how to take it out with precision.
In Tactical Anatomy training we emphasize the need to “see” vital target zones, not just surface land-marks. A tragic tale underscoreing this was related to me by a SWAT commander a few years ago. His sniper had an armed hostage-taker in his sights, using the felon’s ear as his aiming point, as he’d been trained. All the sniper’s training had been on flat ranges, but in this case he was aiming down at a 30 degree angle. When the green light was given his bullet hit his intended surface target, but missed the CNS entirely. The felon was severely wounded, but before he fell he pulled his own trigger, wounding the hostage. That department now faces two lawsuits.
PIECING THINGS TOGETHER
Cops on America’s streets face unprecedented challenges and, as we all know from reading the papers, America’s criminals are increasingly willing to shoot it out. Studies by people like Dr. Bill Lewinski have shown us the offender has the initial advantage in a gunfight because felons initiate the violence and cops react in response. This puts the cop “behind the curve” at the outset of the gunfight.
But by knowing where to place bullets with certainty, cops can overtake the advantage, using their superior knowledge and training to make effective shots to finish the fight decisively.
Teaching the anatomy of the vital target zones gives you the beginnings of that advantage. The next step is hard-wiring that knowledge into our brains through the use of carefully crafted training translating knowledge into effective gunfighting skills. In our third and final installment we’ll discuss hard-wiring 3D anatomic visualization through force-on-force training.